

Here is a fact that should stop you cold. The infant mortality rate in the United States is 5.1 deaths per 1,000 live births, ranking 54th among the 195 countries and territories measured, and significantly higher than dozens of other developed countries, including Sweden at 2.3, Japan at 1.9, and Australia at 2.9, according to the World Population Review.
Think about what that means for a moment. The United States of America, the country that put a man on the moon, that built the internet, that spends more on healthcare than any nation in human history, is losing its babies at a rate that puts it closer to developing nations than to its peers in the industrialized world.
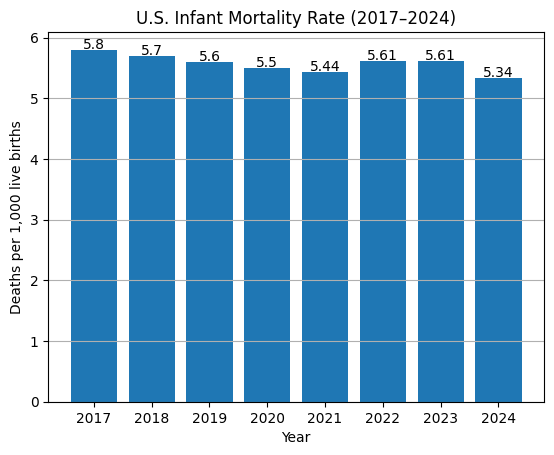
As noted by the CDC, the infant mortality rate was 5.61 deaths per 1,000 live births in 2023, unchanged from the 2022 rate. The increase from 2021 (5.44) to 2022 was the first such rise since the increase from 2001 to 2002. That two-year plateau, after decades of progress, is not a blip. It is a warning siren.
As noted by the Macrotrends historical database, the U.S. infant mortality rate for 2024 was 5.34, a 2.87% decline from 2023’s 5.50 rate. So there is modest improvement on the surface, but the deeper story, as we will see, is one of entrenched disparity, international embarrassment, and political neglect.
The Baseline Numbers, What We Know Right Now

Let’s lay the foundational data on the table so that nobody can claim ignorance.
As noted by the CDC’s Vital Statistics Rapid Release Program, the NCHS presents infant mortality rates based on final mortality data for 2023 and 2024, and provisional mortality data for 2025, with estimates based on all death records received and processed by NCHS as of January 25, 2026.
U.S. Infant Mortality Rate, Historical Trend
Dr. Danielle Ely, co-author of the NCHS report and a health statistician, noted that 2022 was the first year in about 20 years that there was a significant increase in the infant mortality rate, and 2023’s flat result confirmed that it was not just a one-year anomaly, as noted in an ABC News article.
“So what we’re seeing,” she told ABC News, “is that what we were hoping would be just a one-year blip is now a two-year higher rate.”
Two years at an elevated plateau, after two decades of slow progress. Every percentage point represents thousands of families. Every flat trendline is a policy failure, not a statistical abstraction.
Causes of Death: What is Actually Killing These Babies

Before we get to the politics, let us be precise about the medicine. Understanding why infants die is essential to understanding why nothing is changing.
As noted by Worldpopulationreview.com, infant mortality in the United States is predominantly caused by congenital disabilities, preterm birth and low birth weight, maternal pregnancy complications, Sudden Infant Death Syndrome (SIDS), and injuries such as accidental suffocation.
As noted by the March of Dimes 2025 Report Card, only 17 states met the Healthy People 2030 target for infant mortality of 5.0 deaths per 1,000 births. That means 33 states and the District of Columbia are still failing to meet a basic public health benchmark set years ago, a goal that itself is modest by international standards.
Leading Causes of Infant Mortality in the U.S.
Cause of Death
Notes
Congenital disabilities (birth defects)
#1 cause nationally
Preterm birth / Low birth weight
#2 cause; strongly tied to race/poverty
Maternal pregnancy complications
Includes pre-eclampsia, infections
Sudden Infant Death Syndrome (SIDS)
Disproportionately affects Black infants
Unintentional injuries (incl. suffocation)
Includes unsafe sleep environments
As noted in research published by the CDC, for non-Hispanic Black women, 78% of their elevated infant mortality rate compared with non-Hispanic white women was due to their higher percentage of preterm births, while 22% was due to higher gestational age-specific infant mortality rates.
That number, 78% attributable to preterm birth, is perhaps the single most important statistic in understanding the racial gap. It tells us that the disparity is not random.
It has roots in prenatal care access, socioeconomic stress, and systemic healthcare inequities. And those are all things a government can fix, if it chooses to.
The Racial Chasm, America’s Most Damning Statistic
Now here is where you need to sit down, because what follows is not a policy debate. It is a moral emergency.
As noted by ABC News, citing CDC data, Black infants died at a rate of 10.9 infant deaths per 1,000 live births, more than double the rate of 4.5 deaths per 1,000 live births for white women, and more than triple the 3.4 deaths per 1,000 for Asian women. Infants born to American Indian and Alaska Native women had a rate of 9.2 deaths per 1,000 live births.
As noted by the HHS Office of Minority Health, in 2023, the mortality rate for Black/African American infants was 95% higher than for infants nationwide. Black/African American infants were about 2.5 times more likely to die from problems related to being born too early or with low birth weight compared with infants in the U.S. overall.
Furthermore, Black/African American mothers were 49% more likely than mothers nationwide to receive late or no prenatal care.
U.S. Infant Mortality Rate by Maternal Race/Ethnicity (2023)
Racial/Ethnic Group
IMR (per 1,000 live births)
Ratio vs. White
Black/African American
10.9
2.42x
American Indian/Alaska Native
9.2
2.04x
Hispanic
4.8–5.0
~1.1x
White (Non-Hispanic)
4.5
1.0x (baseline)
Asian
3.4–3.5
0.78x
As noted by The Global Statistics, the infant mortality rate of 10.93 deaths per 1,000 live births for Black infants means approximately 1 in 91 Black infants die before their first birthday, compared to roughly 1 in 222 white infants.
This disparity translates to over 2,500 excess Black infant deaths annually that would not occur if Black infants died at white infant rates.
Over two thousand five hundred excess deaths. Every single year. That is not a statistic; that is a catastrophe that has been normalized through decades of political inaction.
As noted by KFF (Kaiser Family Foundation), disparities in infant mortality have persisted and sometimes widened for over a century, particularly between Black and White infants, and research shows that this disparity for Black women increases by age and persists across education and income levels, with Black women who completed college education showing higher pregnancy-related mortality rates than White women with less than a high school diploma.
The State by State Divide, One Nation, Two Realities

America is not one country when it comes to infant mortality. It is a patchwork of wildly different outcomes separated by state lines.
As noted by the 2025 America’s Health Rankings report, New Hampshire had the lowest infant mortality rate in the U.S. at 3.2 deaths per 1,000 live births in 2022–2023, placing it on par with Australia and Germany. The state with the highest rate, Mississippi, had an infant mortality rate of 9.0, more than twice the OECD average.
U.S. Infant Mortality Rate, Best and Worst States
State
IMR (per 1,000 live births)
Performance
New Hampshire
3.2
Best in the U.S.
Massachusetts
~3.94
Top tier
California
~3.92
Top tier
Rhode Island
~3.96
Top tier
Mississippi
9.0
Worst in the U.S.
Louisiana
~7.59
High risk
Arkansas
~7.38
High risk
West Virginia
~7.33
High risk
South Dakota
~7.30
High risk
Mississippi’s rate of 9.0 is not just the worst in America. It is a scandal. As the 2025 Health Rankings noted, Mississippi’s infant mortality rate of 8.4 (a figure now updated to 9.0) is more than twice the OECD average.
This means that being born in Mississippi is, statistically speaking, more dangerous than being born in many countries that the United States considers less developed.
The geographic clustering is not random. The states with the worst outcomes, Mississippi, Louisiana, Arkansas, and West Virginia, share common denominators: high rates of poverty, limited access to prenatal care, significant uninsured populations, and, in many cases, state legislatures that have declined Medicaid expansions that could directly address these gaps.
The International Embarrassment, Richest Country, Worst Outcomes
BREAKING: 🇺🇸 U.S. Infant Mortality Rate rose 3% since 2021 (from 5.44 to 5.6 infant deaths per 1,000 live births) – the largest increase in over two decades according to the CDC.
Infant mortality rate in 2021:
🇲🇨 Monaco: 1
🇸🇲 San Marino: 2
🇪🇪 Estonia: 2
🇯🇵 Japan: 2
🇸🇬…— World of Statistics (@stats_feed) November 1, 2023
This is the part that should produce genuine national shame. Not ideological outrage. Shame.
As noted by the American Journal of Managed Care (AJMC), of all comparable countries in 2020, the United States had the highest infant mortality rate at 5.4 deaths per 1,000 live births, markedly higher than Norway’s 1.6, the lowest in the world.
The U.S. spends 17.8% of gross domestic product on healthcare, nearly twice the average OECD country, yet achieves worse outcomes.
As noted by the 2025 America’s Health Rankings International Comparison, the average infant mortality rate among OECD countries in 2023 was 4.2 deaths per 1,000 live births. At 5.6, the U.S. ranked No. 32 among the 38 OECD countries, falling between New Zealand (4.8) and Chile (6.5). Estonia had the lowest infant mortality rate at 1.7.
To be crystal clear about what these numbers mean: the United States of America spends more per capita on healthcare than any country on earth, and its babies die at a rate closer to Slovakia’s than to Germany’s, France’s, or Japan’s.
That is not bad luck. That is a system producing exactly the results its incentives are designed to produce.
As noted by the Peterson-KFF Health System Tracker, even when adjusted to include only infant deaths meeting a minimum threshold of 22 weeks of gestation or 500g birth weight, to control for different national reporting standards, the U.S. infant mortality rate remains higher than the comparable country average (4.9 vs. 2.9 deaths per 1,000 live births).
So the argument that “the U.S. just counts more deaths” does not hold. Even on an apples-to-apples basis, America is losing.
The Spending Paradox, Money Without Results

As noted by the America’s Health Rankings 2025 report, the United States spent the highest amount per capita on healthcare of all OECD countries, while Switzerland, which ranked No. 2 in health spending, spent only about two-thirds what the U.S. spent per capita.
Roughly 56% of total U.S. health spending came from public funds, well below the OECD average of 73%.
As noted by TIME magazine, citing research published in Health Affairs, if the U.S. had kept pace with the OECD’s overall decline in infant mortality since 1960, that would have resulted in about 300,000 fewer infant deaths over 50 years.
Three hundred thousand. That is the cost of American exceptionalism in infant lives.
The research also offers a pointed diagnosis. As noted by TIME, the U.S. spends more on healthcare, which is taking care of children that are already sick, but far less money on welfare programs to keep children from becoming sick, and on keeping them safe from injuries.
Poverty among U.S. children has been higher than in 19 comparable OECD countries since the mid-1980s, affecting over 20% of American children.
This is the key insight that most healthcare debates miss. The problem is not purely clinical. It is structural.
When more than one in five American children lives in poverty, when prenatal care is rationed by insurance status, and when the social safety net has been systematically dismantled, the consequences show up in maternity wards. They always have.
The Preterm Birth Problem, The Engine of Mortality
View this post on Instagram
No discussion of infant mortality is complete without zeroing in on preterm birth, because it is the single most powerful driver of infant death in America.
As noted by PMC (NIH), preterm births, when a baby is born before 37 weeks of pregnancy, are the second leading cause of infant mortality. The overall preterm birth rate in the United States slightly declined from 10.2% in 2019 to 10.1% in 2020, but when stratified by race, Black and Hispanic populations experience major disparities.
The clinical interventions exist. The problem is access. As noted by a PMC retrospective cohort study, Black women were less likely to receive antenatal corticosteroids (ACS), which accelerate fetal lung development and reduce complications of preterm birth, compared to White patients (37.7% vs. 44.4%). Black women were also less likely to receive respiratory support and surfactant treatment for their infants.
The medicine is available. The treatment works. Black mothers just receive it less. That is a healthcare delivery failure. And it is one with a body count.
2025–2026 Outlook: Where Are We Heading?
As noted by the CDC’s Rapid Release, provisional estimates for 2025 are based on provisional death and birth data, with quarterly updates tracking infant, neonatal, and postneonatal death rates against the five leading causes of death.
The slight decline in 2024 (from 5.61 to 5.34) is encouraging, but it must be kept in context. The global infant mortality rate has dropped from approximately 140 per 1,000 live births in 1950–55 to around 25 in 2025. The U.S. has participated in that global trend, but continues to lag its peer nations in the rate of improvement.
What does 2026 look like? The honest answer is: uncertain, and potentially concerning. Several structural factors are moving in the wrong direction:
Key Risk Factors Driving U.S. Infant Mortality in 2025–2026
Risk Factor
Population Most Affected
Addressable?
Preterm birth
Black women, low-income
Yes, prenatal care, ACS treatment
Late/no prenatal care
Black women (+49%), uninsured
Yes, Medicaid expansion, outreach
Low birth weight
Minority, poverty-affected
Yes, maternal nutrition programs
SIDS
Black, American Indian infants
Partially, safe sleep education
Congenital defects
All groups
Partially, folic acid, genetics
Rural hospital gaps
Rural South, Appalachia
Yes, policy investment
Maternal obesity/chronic disease
All groups, esp. low-income
Yes, preventive care access
Bottom Line
@janai US gets a D+ on #infant mortality report #health #moms #babiesoftiktok #pregnancy ♬ original sound – Janai Norman
Let us be direct. The United States infant mortality crisis is not a mystery. It is not inevitable. It is not even particularly difficult to understand. The solutions are well-documented, widely understood, and implemented effectively by dozens of countries that spend far less money per person.
The discussion, however, has gone on long enough. The data is not ambiguous. The racial gap is not closing. The international ranking is not improving.
More than 20,000 American infants die every year before their first birthday, and a disproportionate number of them are Black, poor, rural, or uninsured. That is not fate. That is policy.
America doesn’t have an infant mortality problem. It has a political will problem. And until the country is willing to confront that with the same urgency it brings to defense budgets and tax legislation, the numbers will continue to tell the same ugly story, year after year, quarter after quarter, one small grave at a time.
References
- CDC NCHS, Infant Mortality in the United States 2023
- CDC Vital Statistics Rapid Release, Infant Mortality Dashboard
- America’s Health Rankings 2025, International Comparison
- KFF, Racial Disparities in Maternal and Infant Health
- HHS Office of Minority Health, Infant Mortality and Black/African Americans
- March of Dimes 2025 Report Card
- World Population Review, Infant Mortality Rate by Country 2026
- AJMC, US Highest Infant Mortality Despite Most Healthcare Spending




