The Ebola outbreak in eastern Democratic Republic of Congo has worsened sharply, with authorities reporting 513 suspected cases and 131 suspected deaths as response teams try to confirm infections, trace contacts, and slow transmission in areas already hit by conflict, displacement, and limited medical access.
The outbreak involves the Bundibugyo species of Ebola, a rarer form of the virus for which there is no approved vaccine, at least for now, and no specific approved treatment. That has raised concern among health officials because many of the tools used in previous Ebola responses were developed for the Zaire strain, which has caused several earlier outbreaks in Congo.
The World Health Organization has warned about the scale and speed of the epidemic. On May 17, the WHO declared the outbreak in Congo and Uganda a Public Health Emergency of International Concern, a designation used for events that require coordinated international action.
WHO also said the outbreak does not meet the criteria for a pandemic emergency. For people outside the affected region, health agencies continue to describe the risk as low, but the situation in eastern Congo has become more serious because cases have appeared in several locations and imported infections have been reported in Uganda.
Latest update: There are over 1000 Cases in Congo.
Case Numbers Have Risen Within Days
The figures have shifted quickly. On May 16, the WHO reported 246 suspected cases and 80 suspected deaths in Ituri province, with eight samples confirmed in laboratory testing. By May 18, the Africa CDC reported about 395 suspected cases and 106 deaths.
On May 19, the Congolese health ministry reported 513 suspected cases and 131 suspected deaths, according to The Associated Press.
Many of those deaths still need laboratory confirmation or further investigation. In an outbreak of this kind, early numbers can change as health teams reach communities, review medical histories, and test samples. Still, the rise in suspected cases has been rapid enough to prompt warnings from international health agencies.
Confirmed or suspected cases have been reported in Bunia, Mongbwalu, Rwampara, Butembo, Nyakunde, and Goma. Uganda has also reported imported cases involving people who traveled from Congo, including one death in Kampala, according to WHO updates.
Why the Outbreak Has Alarmed Health Officials
The first known suspected case was a health worker who developed symptoms on April 24 and later died at a medical center in Bunia. The body was then taken to Mongbwalu, a mining area where people move in and out for work and trade. That movement has made the early investigation harder.
Ebola spreads through direct contact with infected bodily fluids. Funerals, body transport, and care for sick relatives can create high-risk exposure when safe burial and infection-control measures are not in place.
View this post on Instagram
Early testing also complicated the response. Initial samples were tested for the Zaire strain and came back negative. Later testing at the National Institute of Biomedical Research in Kinshasa confirmed the Bundibugyo virus. That delay may have allowed the outbreak to grow before health authorities understood which Ebola species they were dealing with.
Health workers have also been affected. WHO said the first alert on May 5 involved a high-fatality illness in Mongbwalu, with deaths among medical staff. Infections among medical workers can put clinics under pressure, reduce available care, and increase the risk of transmission in health facilities.
In a Washington Post opinion piece, Leana S. Wen warned that the outbreak had received too little attention compared with other health threats. Her argument focused on the severity of Ebola, the lack of approved countermeasures for Bundibugyo, and the danger created by delayed detection.
How Bundibugyo Ebola Spreads?
Ebola does not spread through the air in the way measles or COVID-19 can. Bundibugyo virus spreads through direct contact with blood, vomit, diarrhea, saliva, semen, organs or other bodily fluids from an infected person, or from someone who died of the disease. Contaminated clothing, bedding, medical equipment, and burial materials can also carry the virus.
WHO says the incubation period ranges from 2 to 21 days. People usually become infectious only after symptoms begin. Early symptoms can include fever, fatigue, muscle pain, headache, and sore throat. Later illness can involve vomiting, diarrhea, abdominal pain, organ failure, and, in severe cases, bleeding.
Previous Bundibugyo outbreaks have had fatality rates of roughly 30% to 50%, according to WHO. Outcomes can vary depending on how early patients receive care, how quickly contacts are traced, and whether treatment centers can provide fluids, monitoring, and management of complications.
Why Congo and Uganda Are Central to The Response
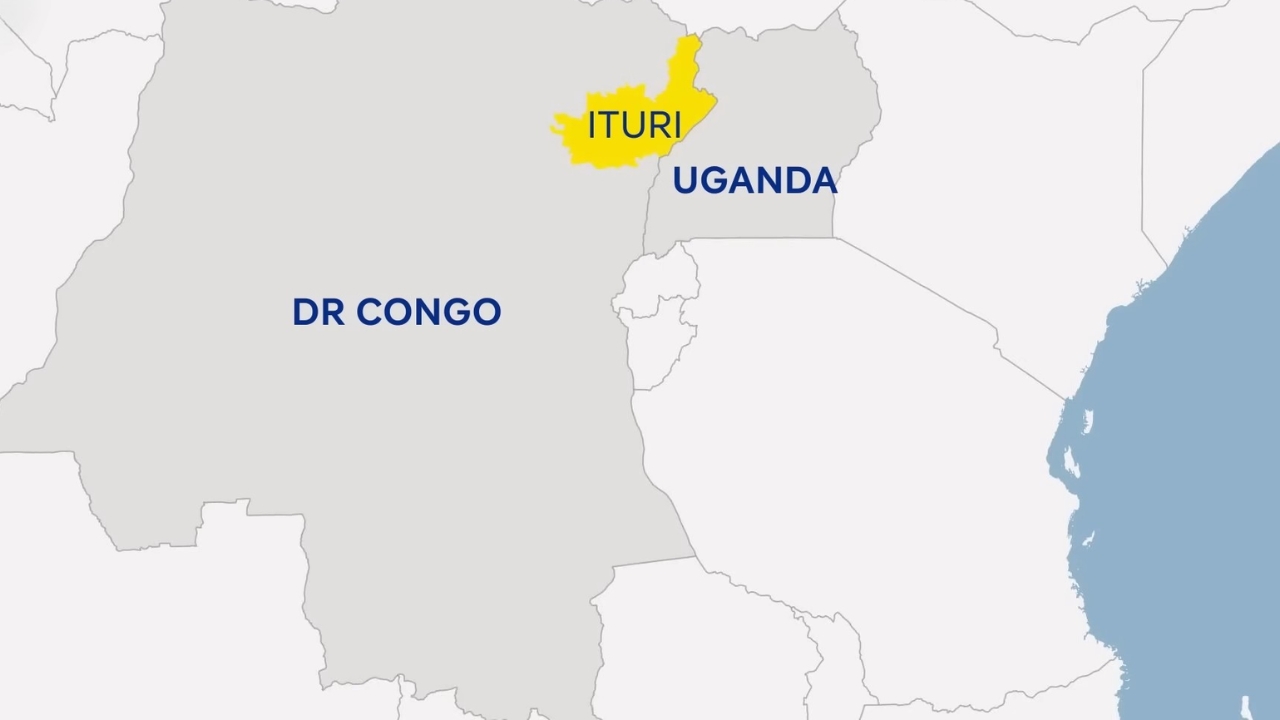
The affected part of eastern Congo sits near busy movement routes. Ituri province borders Uganda and South Sudan, while Bunia serves as a commercial hub. Mongbwalu is a mining area, and mining-linked travel can make contact tracing more difficult because workers, traders, and families may move between towns before symptoms become clear.
Security conditions add another problem. Ituri and nearby North Kivu have faced prolonged armed violence and population displacement. WHO has warned that insecurity can delay sample collection, restrict safe access for health teams, and weaken follow-up with people who may have been exposed.
Uganda has confirmed imported Bundibugyo cases after people traveled from Congo. Health authorities there have activated surveillance, screening, and response measures. Africa CDC has called for regional coordination involving DRC, Uganda, South Sudan, WHO, UNICEF, U.S. CDC, and other partners.
Emergency Declarations and Response Measures
WHO declared the outbreak a Public Health Emergency of International Concern on May 17. The declaration is meant to support international coordination, faster resource mobilization, and closer reporting under global health rules.
Africa CDC also declared the outbreak a Public Health Emergency of Continental Security on May 18. The agency cited cross-border movement, insecurity, weak infection prevention, and community deaths outside health facilities as major concerns.
Response measures now include isolation of suspected and confirmed cases, contact tracing, safe burials, community outreach, laboratory sequencing, infection prevention in health facilities, and border screening.
WHO said rapid response teams, medical supplies, and treatment capacity are being deployed. CDC said its support includes disease tracking, contact tracing, laboratory work, sequencing, and infection-control guidance.
American Doctor Infected as U.S. Screening Expands
The US Centers for Disease Control and Prevention says that one American national has contracted Ebola “as part of their work in the Democratic Republic of Congo”; CDC’s Ebola response incident manager Satish Pillai stated on Monday: “The person developed symptoms over the… pic.twitter.com/PPg8Qc65pU
— TRT Afrika (@trtafrika) May 18, 2026
A U.S. citizen working as a doctor in Congo tested positive for Ebola after caring for patients, according to CDC and Congolese officials. CDC said the patient and high-risk contacts were being moved to Germany for care and monitoring because Germany has experience treating Ebola patients, and the flight is shorter.
On May 18, the CDC and the Department of Homeland Security began enhanced travel screening, entry restrictions, and public health measures for people arriving from DRC, Uganda, and South Sudan. CDC says no outbreak-linked Ebola cases have been confirmed in the United States, and the overall risk to the American public remains low.
CDC has also issued a Level 3 travel notice for affected areas in DRC, advising people to reconsider nonessential travel to Ituri and North Kivu provinces.
Travelers who must go to affected areas are advised to avoid contact with sick people, bodily fluids, health facilities in affected zones, traditional healers, dead bodies, funeral practices involving body contact, caves, mines, bats, forest antelopes, and nonhuman primates.
What Makes the Bundibugyo Strain Harder to Contain?
Congo has dealt with Ebola before, but the most recent response experience has involved the Zaire strain. That strain has approved vaccines and antibody treatments. Bundibugyo does not.
Supportive care can still improve survival. Patients need fluids, monitoring, treatment for secondary infections, and management of organ complications. The lack of a licensed vaccine or specific approved treatment means response teams have less room for delay.
Testing also becomes more complicated. Rapid tests designed around the Zaire Ebola can miss Bundibugyo infections. That appears to have contributed to the delay between the first suspected illness in late April and laboratory confirmation in mid-May.
Bundibugyo has been recorded less often than other Ebola species. WHO notes previous Bundibugyo outbreaks in Uganda in 2007 and the DRC in 2012. Because outbreaks have been limited, health agencies have less operational evidence to draw from than they did for the Zaire Ebola outbreak.
Risk for The Wider Public Remains Low Outside the Outbreak Area
For people outside the affected region, Ebola does not pose the same kind of general public risk as airborne respiratory viruses. Transmission requires direct contact with infectious bodily fluids, contaminated materials, or infected animals.
The highest-risk settings are households caring for sick relatives, health facilities without proper infection-control measures, and burial situations involving contact with the body of someone who died from Ebola.
Travelers who have recently been in affected areas should monitor for fever, headache, muscle pain, weakness, diarrhea, vomiting, stomach pain, or unexplained bleeding for 21 days after leaving. Anyone with symptoms after possible exposure should isolate and contact health authorities before going to a clinic or hospital.
The Next Phase Depends on Speed
@aljazeeraenglish An Ebola outbreak caused by the rare Bundibugyo strain has killed dozens in Democratic Republic of the Congo and is spreading into Uganda, raising fears of regional transmission. . Health officials say instability and shared borders are complicating containment efforts as the World Health Organization declares a global health emergency. #news ♬ original sound – Al Jazeera English
The outbreak is now a test of speed, access, and coordination. Health teams need to confirm cases, identify contacts, isolate patients, and carry out safe burials in communities where insecurity and movement make field work difficult.
Uganda will also remain under close watch. WHO said no local transmission had been identified there at the time of its disease outbreak update, but Kampala is a major transport hub, and imported cases require careful follow-up.
A fast regional response can still prevent wider spread, but delayed detection, health worker infections, urban exposure, insecurity, and the absence of approved Bundibugyo-specific countermeasures have left health agencies with a limited margin for error.