

The U.S. Supreme Court’s decision in Dobbs v. Jackson Women’s Health Organization (June 2022) returned control over abortion regulation to the states. In the four years since, a patchwork of policies has emerged across the country.
As of February 2026, thirteen states enforce near‑total bans on abortion, four states prohibit the procedure at roughly six weeks’ gestation, and several others impose bans after 11–18 weeks.
Meanwhile, voters in nearly a dozen states amended their constitutions to protect reproductive rights, and litigation continues to shape access.
Key Takeaways
New Releases and Emerging Issues
Infant mortality and births increased in most states with abortion bans, studies findhttps://t.co/AXLPimESSS
— TIME (@TIME) February 16, 2025
Numerous research reports and policy briefs have emerged since 2024. Johns Hopkins Bloomberg School of Public Health published two studies in February 2025 evaluating the impact of bans on births and infant deaths.
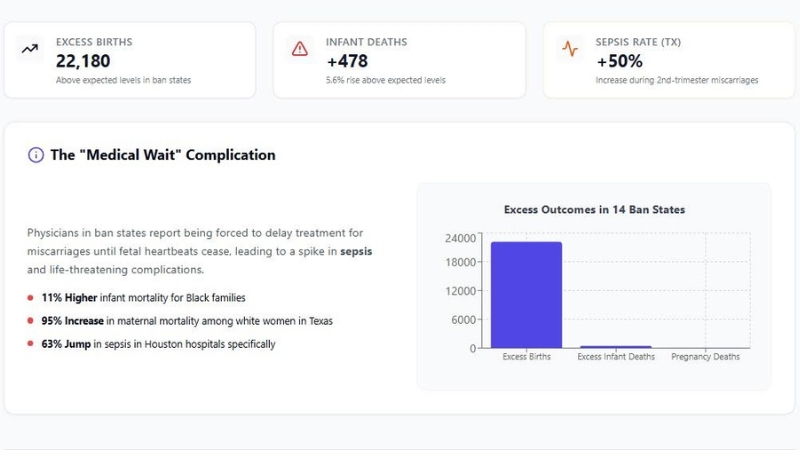
The researchers estimated that abortion bans in 14 states led to 22 180 additional live births and 478 additional infant deaths during the first year after bans took effect. The additional births occurred disproportionately among racially minoritised people, Medicaid beneficiaries, unmarried and younger individuals, and residents of southern states.
Black infants in ban states died at a rate 11 % higher than would have been expected.
Public health organisations have also warned about a spike in pregnancy‑associated complications.
The Population Reference Bureau (PRB) reported in August 2025 that states with abortion bans experienced over 22 000 extra births, 478 excess infant deaths, and 59 pregnancy‑associated deaths, reflecting a public‑health emergency.
Texas, which implemented a six‑week ban in 2021, saw a 50 % jump in sepsis rates among women hospitalised during second‑trimester miscarriages.
The PRB noted that legal uncertainties have forced physicians to delay treatment until fetal heartbeats cease, leading to life‑threatening complications.
Policy watchers have highlighted multiple Supreme Court cases scheduled for 2024–25 that will influence access going forward.
These include Moyle v. United States, which tests whether federal emergency‑care requirements override state abortion bans, and FDA v. Alliance for Hippocratic Medicine, which challenges the Food and Drug Administration’s approval of mifepristone (used in medication abortion).
Federal courts are also being asked to interpret the 1873 Comstock Act, which anti‑abortion advocates cite as a basis for banning the mailing of abortion pills. States continue to enact so‑called “shield” laws protecting providers who mail pills into ban states and to broaden telehealth access.
Legal Landscape: States Where Abortion Is Illegal

Total Bans and Exceptions
By February 2026, 13 states have enacted near‑total abortion bans, leaving the procedure legal only in limited circumstances (usually to save the pregnant person’s life).
West Virginia, the most recent state to join this group, fully banned abortion in September 2022; North Dakota’s ban took effect after the state supreme court lifted an injunction in November 2025, according to the Reproductive Rights.
The table below lists each state, the type of ban, and the narrow exceptions that remain.
State (2026)
Type of ban
Narrow exceptions
Alabama
Total ban
Only to preserve the life of the pregnant person.
Arkansas
Total ban
Only to preserve life.
Idaho
Total ban
Life‑saving; survivors of rape/incest must report to law enforcement; a physician may act if pregnancy poses a non‑negligible risk of death.
Indiana
Total ban
Exceptions for lethal fetal anomaly, rape or incest before 12 weeks, or serious risk to health or life.
Kentucky
Total ban
To preserve life or health.
Louisiana
Total ban
To preserve life or for a lethal fetal anomaly.
Mississippi
Total ban
Survivors of rape or incest (must report); life‑saving.
North Dakota
Total ban
Death or serious health risk to the pregnant person; rape or incest up to six weeks.
Oklahoma
Total ban
No explicit exceptions; physicians face felony penalties.
South Dakota
Total ban
Only to preserve life.
Tennessee
Total ban
Life‑saving or to prevent a serious health risk.
Texas
Total ban
Limited medical emergencies; physicians risk felony charges.
West Virginia
Total ban
Exceptions for non‑viable pregnancy, ectopic pregnancy, or survivors of rape/incest (8–14 weeks) who have reported the incident.
These bans make no provision for preserving fertility, maternal health, or severe fetal anomalies (except in a few states), forcing many residents to travel across state lines.
Because rape and incest exceptions often require survivors to file police reports and meet narrow time limits, they are rarely used in practice.
In states such as Oklahoma and Texas, physicians face felony penalties and civil lawsuits for performing abortions.
Early Gestational Bans and Bans After Conception
Four states prohibit abortion at roughly six weeks’ gestation, before many people know they are pregnant.
View this post on Instagram
Georgia, South Carolina, Florida, and Iowa enforce six‑week bans with exceptions for medical emergencies and, in some cases, rape/incest when reported to law enforcement. Florida’s law allows rape, incest, domestic violence, or human‑trafficking survivors to access abortion until 15 weeks with documentation.
In North Carolina, a new law (May 2023) bans abortion after 12 weeks, with exceptions for rape or incest through week 20 and lethal fetal anomalies through week 24.
Nebraska bans abortion after 11 weeks and 6 days, and Utah bans the procedure after 18 weeks. Laws in Wisconsin (22 weeks) and other states restrict abortion at viability or 24 weeks.
The Guardian’s interactive tracker, updated 12 January 2026, notes that 13 states have enacted near‑total bans, and four states, Georgia, South Carolina, Florida, and Iowa, ban abortion past approximately six weeks.
It also describes states “in flux,” including Missouri, where litigation has delayed implementation of a voter‑approved 2024 amendment protecting abortion rights; a competing measure to reinstate the ban will appear on the 2026 ballot.
Protective States
In contrast, more than half of U.S. states have enacted laws protecting abortion rights. According to the Center for Reproductive Rights, 25 states and Washington, D.C. have legal protections, while the remaining states maintain bans or restrictions.
States such as California, Colorado, Connecticut, and Minnesota permit abortion without gestational limits. Others (e.g., Illinois, Maryland, New York) allow abortion until viability, typically around 24 weeks, with exceptions to preserve the patient’s life or health.
Ballot Measures and Political Action
2024 Ballot Results
The 2024 election cycle saw an unprecedented number of abortion‑related ballot measures. Voters in Arizona, Colorado, Maryland, Missouri, Montana, New York, and Nevada approved constitutional amendments protecting abortion rights.
Conversely, voters in Florida, Nebraska, and South Dakota rejected similar proposals, with Nebraska approving a competing measure to ban abortions after the first trimester.
Looking Ahead To 2026
By early 2026, two ballot measures will be certified for the upcoming elections. Missouri Amendment 3 would overturn the 2024 amendment and ban abortion except for medical emergencies, fetal anomalies, and narrowly defined rape/incest, while also restricting gender transition surgeries for minors.
Nevada will vote a second time on its constitutional amendment because the state requires two consecutive approvals to amend the constitution.
Proposed initiatives are underway in Idaho, Montana, Nebraska, Oregon, and Virginia to enshrine reproductive freedom or to declare fetal personhood. Ballot measures have become central to abortion policy: KFF notes that only a handful of ban states allow citizen‑initiated constitutional amendments, limiting avenues for overturning bans.
Key Facts and Statistics
The legal landscape intersects with shifting abortion trends. According to the Guttmacher Institute, 13 states have total bans, and six states restrict abortion between 6 and 12 weeks.
KFF reports that national abortion numbers rose after Dobbs: there were 1.14 million abortions in 2024, with 591 770 in the first half of 2025; the monthly average increased from 79 620 in 2022 to 98 630 in early 2025, reflecting telehealth availability, shield laws, and interstate travel. The table below summarises key metrics.
Indicator (United States)
Value & source
Total abortions (2024)
1 142 970 procedures.
Average abortions per month
79 620 in 2022 vs. 98 630 (Jan–Jun 2025).
Share of abortions via medication (2023)
63 %.
Abortions by gestational age (2022)
78.6 % at ≤ 9 weeks and 92.8 % at ≤ 13 weeks.
First‑trimester abortions
93 % of abortions occur in the first trimester.
Age distribution (2022)
57 % of abortion patients were in their twenties.
Racial distribution (2022)
40 % of abortions were among Black women, 32 % among White women, 21 % among Hispanic women, and 7 % among women of other races.
Medication-abortion success & safety
Success rate of 99.6 %; risk of major complications 0.4 %; mortality rate <0.001 %.
Median cost (2023)
Medication abortion: $563; procedural abortion: $650; telehealth medication abortion: ~$150.
Insurance coverage
Only 11 % of patients used private insurance, and 26 % used Medicaid; 60 % paid out‑of‑pocket.
Medication Abortion

Medication abortion, a two‑drug regimen of mifepristone and misoprostol, is the most common method of terminating pregnancies in the United States.
The regimen is approved by the FDA up to 10 weeks’ gestation and is endorsed by the World Health Organisation up to 12 weeks, according to KFF. In 2023, 63 % of U.S. abortions were performed with medication, and more than a quarter were accessed via telehealth.
Mifepristone is taken first to block progesterone, followed by misoprostol 24–48 hours later to induce uterine contractions; a misoprostol‑only regimen is used in many countries but is not approved in the U.S.
Safety and efficacy: The medication‑abortion protocol has a 99.6 % success rate and a major‑complication rate of 0.4 %. Major complications are rare and typically involve incomplete abortions requiring a procedural intervention. The risk of death from medication abortion is less than 1 per 100 000 cases.
By comparison, the risk of death during childbirth is far higher, particularly in states with abortion bans (see Related Health below).
Legal and regulatory issues: Several states require in‑person dispensing of Mifepristone, ban telehealth prescriptions, or restrict mailing of pills. The Supreme Court will hear FDA v. Alliance for Hippocratic Medicine in 2024–25, a case that could overturn the FDA’s approval of mifepristone and restrict telehealth.
Anti‑abortion advocates also cite the 19th‑century Comstock Act to argue that mailing abortion pills is illegal; the Biden administration contends that the law does not apply to consensual medical services.
In response to these challenges, states such as Colorado and Massachusetts have enacted shield laws protecting clinicians who prescribe and mail medication abortion across state lines.
Coverage and Cost
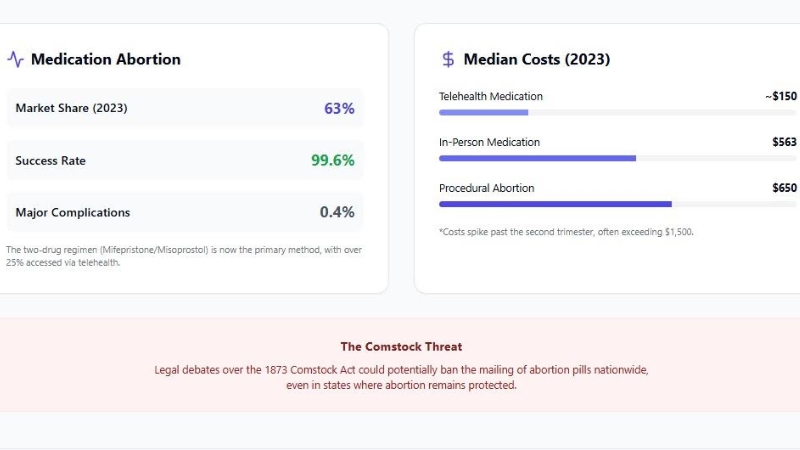
Abortion costs vary widely, and insurance coverage is inconsistent. The median price for a medication abortion was $563 in 2023, while a procedural abortion cost $650. Virtual‑clinic medication abortions typically cost around $150. Costs increase later in pregnancy; second‑trimester procedures often exceed $1 500 and require travel to specialised clinics.
Insurance: Federal law (the Hyde Amendment) prohibits the use of federal funds for abortion except in cases of rape, incest, or life endangerment, limiting Medicaid coverage. Consequently, 20 states use their own funds to cover abortions beyond federal restrictions.
Conversely, 10 states restrict abortion coverage in private insurance plans, and 25 ban it in Marketplace plans. Only 12 states require private plans to cover abortion, and nine require no cost‑sharing.
As a result, 60 % of abortion patients pay out‑of‑pocket, while just 11 % use private insurance and 26 % rely on Medicaid. Abortion funds and practical‑support organisations provide financial assistance and report dramatic increases in requests since Dobbs.
Related Health Outcomes
Evidence is mounting that abortion bans have serious health consequences beyond restricting the procedure.
Maternal mortality has diverged sharply between states with and without bans.
The Gender Equity Policy Institute observed that maternal mortality fell 21 % in supportive states but rose 56 % overall and 95 % among white women in Texas during the first year of its six‑week ban. Black mothers in ban states were 3.3 times more likely to die during pregnancy or postpartum than white mothers.
The Milbank Memorial Fund summarized research indicating that restrictive policies have increased birth rates by roughly 2 % above trend predictions and are associated with shortages of obstetric providers.
Nearly 40 % of OB/GYN practitioners in ban states report new constraints on treating miscarriages and pregnancy emergencies, and 55 % say their ability to follow medical standards has been compromised. Because of unclear exceptions, physicians may delay care until a patient is critically ill.
Studies from Johns Hopkins show that bans led to 22 180 additional births and 478 additional infant deaths across 14 states, with fertility rates rising 1.7 % over expected levels. The PRB likewise reported 22 000 extra births, 478 excess infant deaths, and 59 pregnancy‑associated deaths.
Texas experienced a 50 % increase in sepsis rates among women hospitalised during second‑trimester miscarriages, and hospitals in Houston recorded a 63 % jump in sepsis after the six‑week ban.
The increased infant mortality was disproportionately borne by Black infants, whose mortality rate rose 11 % compared with 5 % for white infants.
Racial & Ethnic Disparities

Abortion bans exacerbate long‑standing racial and ethnic disparities in reproductive health. CDC surveillance data from 2022 show that non‑Hispanic Black women accounted for 39.5 % of abortions, while non‑Hispanic White women accounted for 31.9 % and Hispanic women 21.2 %.
Black women had the highest abortion rate (24.4 per 1 000 women) and a high abortion ratio (429 abortions per 1 000 live births). More than 78 % of abortions occurred at ≤ 9 weeks and 92.8 % at ≤ 13 weeks.
Post‑Dobbs research indicates that bans disproportionately increase births among racially minoritised groups. Johns Hopkins estimated that fertility rates in ban states rose about 2 % among non‑Hispanic Black, Hispanic, and “other” races and ethnicities, compared with 0.3 – 2.3 % overall.
The PRB found that Black infants experienced an 11 % rise in mortality after bans. GEPI data show that Black mothers in ban states are 3.3 times more likely to die during pregnancy or postpartum than white mothers, while Latina mothers in Texas face nearly triple the risk compared with their counterparts in California.
These disparities underscore how restrictive policies amplify structural racism and socioeconomic inequality.
State Data
While national trends are informative, outcomes vary dramatically by state. Texas accounted for 75 % of the excess births attributable to bans, largely because it implemented its six‑week ban earlier than other states.
Kentucky and Mississippi each saw fertility increases of about 1.4 %. States with strong protections, such as California and New York, continue to provide high volumes of care to residents from ban states. KFF estimates that 155 000 women from ban states obtained abortions in other states in 2024.
Conversely, some ban states report zero legal abortions, illustrating how access has vanished locally. In supportive states, birth rates have declined or remained stable despite an influx of patients from restrictive states.
For example, the Gender Equity Policy Institute found that maternal mortality fell 21 % in supportive states after the Dobbs decision.
Public Opinion and Polling
Public opinion remains more supportive of abortion rights than the legal landscape might suggest.
A KFF Women’s Health Survey (Jan 2026) found that 70 % of women of reproductive age support a nationwide right to abortion, with 88 % supporting access when a pregnant person’s life is at risk, 79 % supporting the ability to travel to obtain an abortion, and 67 % supporting protections for doctors who provide abortions.
An AP‑NORC poll (July 2025) reported that 64 % of Americans believe abortion should be legal in all or most cases, while 36 % think it should be illegal in all or most cases. Support varies by party: 85 % of Democrats favour legal abortion, compared with 41 % of Independents and 32 % of Republicans.
Pew Research Center’s 2025 state‑level survey found that in 34 states and Washington D.C., more residents say abortion should be legal in all or most cases than say it should be illegal; only Arkansas showed a majority favouring illegality. In the District of Columbia, 81 % of adults support legal abortion.
Conclusion
@nytimes In the year since Roe fell, 20 states have enacted laws banning or restricting abortion, forcing a rapid shift in the country’s patchwork of abortion access. Clinic owners scrambled to adjust, canceling appointments and helping patients travel elsewhere. Some clinics relocated, while others stayed open to provide the services they still could. Many simply closed. The reporters Allison McCann and Amy Schoenfeld Walker traveled to abortion clinics across the country to see what happened to them and the surrounding communities. #roevwade #dobbs #scotus #abortion #abortionclinics ♬ original sound – The New York Times
The landscape of abortion in 2026 is defined by stark contrasts. Thirteen states enforce near‑total bans, often with narrow or impractical exceptions, while four others prohibit the procedure at about six weeks of pregnancy.
Ballot initiatives have become a primary tool for codifying protections or reinstating bans, with high‑stakes votes scheduled in Missouri and Nevada.
Despite the prohibitions, the number of abortions nationwide has increased because residents travel across state lines and access telehealth services. Medication abortion now accounts for nearly two‑thirds of all procedures, and debates over its regulation will reach the Supreme Court.
Emerging research reveals that abortion bans have far‑reaching health consequences: they increase births, infant deaths, maternal mortality, sepsis,s and other complications, with disproportionate impacts on Black and Hispanic communities. The bans also strain obstetric practices and exacerbate regional inequalities.
Public opinion, however, remains largely supportive of legal abortion, suggesting a disconnect between state policies and the preferences of most Americans. Understanding this complex landscape is essential for policymakers, healthcare providers, and voters as they navigate upcoming elections and court decisions.





