The legal status of abortion in the United States now depends almost entirely on state law.
Since the U.S. Supreme Court overturned Roe v. Wade in Dobbs v. Jackson Women’s Health Organization in June 2022, states have moved in opposite directions. Some ban abortion with narrow exceptions. Others protect abortion through state statutes, court rulings or constitutional amendments.
As of the latest KFF state policy data used for this update, 13 states ban abortion, 28 states enforce gestational limits, and 9 states plus Washington, D.C. have no gestational limit. The most restrictive states are concentrated in the South and parts of the Midwest.
The phrase “illegal” needs careful reading. In most ban states, abortion is not available as routine medical care, but statutes still list narrow exceptions for life, physical health, rape, incest or fetal anomalies. Those exceptions differ sharply by state. In practice, they can also be hard to use because hospitals, doctors and patients must operate under criminal, civil and licensing pressure.
This guide breaks down where abortion is banned in 2026, where early limits apply, where access remains broader, and why medication abortion, telehealth, insurance rules, travel and ballot measures now matter as much as the state-by-state ban list.
Here Are the US States Where Abortion Is Illegal in 2026

Thirteen states ban abortion, though most include limited exceptions for life, physical health, rape, incest, lethal fetal anomalies or similar circumstances. The details vary by state. A ban does not mean every pregnancy-related emergency is handled the same way in every hospital or under every statute.
Readers should also note the difference between a legal exception and practical access. A state can list an exception on paper, yet patients may still face delays, transfers, extra documentation, provider uncertainty or a lack of nearby hospitals willing to provide care.
State
Main Exceptions Listed In KFF State Policy Data
What Readers Should Know
Alabama
Life, health and lethal fetal anomalies
One of the most restrictive states after Dobbs
Arkansas
Life
Abortion access inside the state is extremely limited
Idaho
Life, rape or incest in the first trimester
Emergency-care questions remain part of the legal fight
Indiana
Life, physical health, rape or incest up to 12 weeks LMP, lethal fetal anomalies up to 22 weeks LMP
The state has narrow exception windows and strict provider rules
Kentucky
Life and physical health
Voters rejected a 2022 constitutional amendment that would have said there is no state right to abortion, but the ban remains in effect
Louisiana
Life and physical health
The state is also central to 2026 mifepristone litigation
Mississippi
Life and rape up to 6 weeks LMP
The Dobbs case came from Mississippi and ended the federal Roe standard
North Dakota
Life, physical health, rape or incest up to 6 weeks LMP
The state appears in KFF data as a ban state in 2026
Oklahoma
Life
Multiple overlapping abortion restrictions make access extremely limited
South Dakota
Life
Voters rejected a 2024 abortion-rights measure
Tennessee
Life and physical health
Physicians face criminal-law pressure under the state ban
Texas
Life
Texas ban enforcement and private civil actions have shaped the national access map
West Virginia
Life, physical health, rape or incest up to 8 weeks LMP for adults and 14 weeks LMP for minors, lethal fetal anomalies
The state allows limited exceptions but no broad abortion access
The most important correction for 2026 is Missouri. KFF lists Missouri under fetal viability, not as a current total-ban state. Missouri voters approved a reproductive freedom amendment in 2024, clinics later won court relief to resume care, and voters will face another abortion measure in November 2026 that could roll back those protections.
What Are Gestational Limits?
State abortion laws often use “LMP,” meaning last menstrual period. That measure usually dates pregnancy from the first day of the last menstrual period, not from conception. As a result, a six-week LMP law can apply roughly two weeks after a missed period for many patients.
The category also matters. A total ban, a six-week limit, a 12-week limit, a viability standard and a state with no gestational limit are not the same legal situation. The effect on patients can still overlap because appointments, mandatory waiting periods, travel, cost and diagnosis timing all affect access.
| Legal Category | What It Usually Means For Patients |
| Total ban | Routine abortion care is unavailable inside the state, except for narrow listed exceptions |
| Six-week limit | Many patients run out of time before they know they are pregnant or can get an appointment |
| 12-week limit | Some early care remains available, but delays can still close the legal window |
| Viability limit | Care is generally allowed until fetal viability, with exceptions after that point |
| No gestational limit | The state does not set a cutoff, but clinic capacity and provider rules still matter |
States With Six-Week Abortion Bans In 2026
Four states ban abortion at roughly six weeks LMP, a point before many people know they are pregnant. These are not total bans in the same legal category as Alabama or Texas, but they sharply reduce in-state access.
| State | Limit | Main Exceptions Listed In KFF State Policy Data | 2026 Access Effect |
| Florida | 6 weeks LMP | Life, physical health, rape or incest up to 15 weeks LMP, lethal fetal anomalies during the first two trimesters | Florida no longer functions as the major Southern access point it was before the six-week law |
| Georgia | 6 weeks LMP | Life, physical health, rape or incest up to 22 weeks LMP, lethal fetal anomalies up to 22 weeks LMP | The law affects a large state with a major Atlanta metro population |
| Iowa | 6 weeks LMP | Life, physical health, rape or incest up to 22 weeks LMP, lethal fetal anomalies up to 22 weeks LMP | The six-week limit changed access in the Midwest |
| South Carolina | 6 weeks LMP | Life, physical health, rape or incest up to 12 weeks LMP, lethal fetal anomalies | The state remains one of the early-ban states in the Southeast |
The six-week category is important because it can look less severe than a total ban on paper, yet still close off most in-state abortions. A patient who discovers a pregnancy after a missed period, waits for an appointment, faces mandatory delays or needs money for care can run out of legal time quickly.
Other States With Early Or Mid-Pregnancy Limits
Several states allow abortion beyond six weeks but restrict access earlier than viability or before the third trimester. These states sit between the total-ban states and the states with broad legal protections.
| State | 2026 Limit Listed By KFF | Main Exceptions |
| Nebraska | 12 weeks LMP | Life, physical health, rape or incest |
| North Carolina | 12 weeks LMP | Life, physical health, rape or incest up to 20 weeks LMP, lethal fetal anomalies up to 24 weeks LMP |
| Utah | 18 weeks LMP | Life, physical health and fatal fetal anomaly |
| Kansas | 22 weeks LMP | Life and physical health |
| Ohio | 22 weeks LMP | Life and physical health |
| Wisconsin | 22 weeks LMP | Life and physical health |
| Massachusetts | 24 weeks LMP | Life, health and grave fetal anomaly |
| Nevada | 24 weeks LMP | Life and health |
| New Hampshire | 24 weeks LMP | Life, health and lethal fetal anomalies |
| Pennsylvania | 24 weeks LMP | Life and physical health |
| Virginia | Third trimester | Life and health |
Gestational limits are not all the same. A 22-week limit functions differently from a 12-week limit, especially for patients who face delayed diagnosis, fetal anomaly testing, intimate partner violence, unstable housing, immigration barriers, limited money or long travel distances.
States With No Gestational Limit In 2026
KFF lists 9 states plus Washington, D.C. as having no gestational limit. That does not mean every clinic provides care at every stage of pregnancy. It means the state does not set a gestational cutoff in the way other states do.
| State Or District | 2026 Status | What It Means |
| Alaska | No gestational limit | Access still depends on provider availability and geography |
| Colorado | No gestational limit | Major access state for patients traveling from restrictive states |
| District of Columbia | No gestational limit | Important regional access point |
| Maryland | No gestational limit | State has constitutional protection approved by voters in 2024 |
| Michigan | No gestational limit | Voters protected reproductive freedom in 2022 |
| Minnesota | No gestational limit | Upper Midwest access state |
| New Jersey | No gestational limit | Broad legal protection |
| New Mexico | No gestational limit | Major access state for patients from Texas and nearby states |
| Oregon | No gestational limit | Broad legal protection |
| Vermont | No gestational limit | State constitutional protection for reproductive autonomy |
States with no gestational limit still differ in clinic capacity, cost, waiting times, insurance rules and travel needs. Legal permission does not automatically create nearby care.
Medication Abortion Remains The Center Of The Legal Fight

Medication abortion usually refers to a two-drug regimen of mifepristone and misoprostol. KFF says the FDA-approved regimen can be used through 10 weeks of pregnancy, while the World Health Organization authorizes use through 12 weeks.
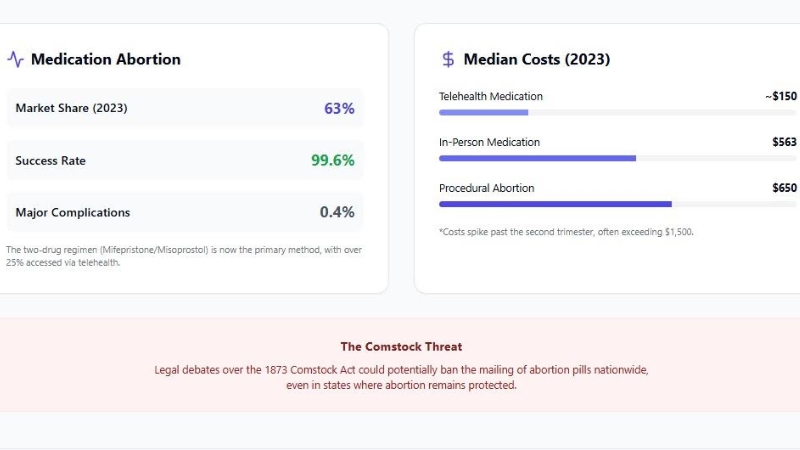
KFF reports that medication abortion accounted for 63% of U.S. abortions in 2023. In the first half of 2025, 27% of all abortions were provided through telehealth.
The legal fight in 2026 centers on mifepristone distribution.
On May 14, 2026, the U.S. Supreme Court blocked a lower-court order in Louisiana v. FDA that would have restricted nationwide mifepristone distribution.
That action left current FDA rules in place, allowing the drug to be prescribed through telehealth and dispensed by mail or retail pharmacies while litigation continues.
| Medication Abortion Fact | Latest Reliable Figure Or Rule |
| Common regimen | Mifepristone followed by misoprostol |
| FDA-approved timing | Up to 70 days, or 10 weeks, of pregnancy |
| Share of U.S. abortions | 63% in 2023 |
| Telehealth share | 27% of all abortions in the first half of 2025 |
| Effectiveness | 91.9% to 99.7% in KFF summary of medication abortion evidence |
| Major complication risk | 0.4% in KFF summary |
| Mortality rate | Less than 0.001% in KFF summary |
| Main 2026 legal issue | Whether federal FDA rules allowing mail and telehealth distribution remain protected from state-led challenges |
State bans apply to medication abortion as well as procedural abortion. In ban states, in-state providers generally cannot legally provide abortion pills except under narrow exceptions. The newer access route comes from clinicians in states with shield laws who provide telehealth care to patients in restrictive states.
Telehealth And Shield Laws Changed The Access Map
Guttmacher’s 2026 release shows how access has shifted. The total number of clinician-provided abortions stayed nearly unchanged from 2024 to 2025, but the route to care changed.
| Abortion Access Measure | 2024 | 2025 | Change |
| Estimated clinician-provided abortions in the U.S. | 1,124,000 | 1,126,000 | Nearly flat |
| Abortions in states without total bans | 1,049,000 | 1,036,000 | Slight decline |
| Telehealth provision to people in total-ban states | 74,000 | 91,000 | Increase |
| People who traveled out of state for abortion care | 154,000 | 142,000 | Decline |
| People from total-ban states who traveled out of state | 74,000 | 62,000 | Decline |
The shift does not mean travel is no longer needed. Guttmacher still describes travel as a major access route, especially later in pregnancy and in cases where telehealth is not appropriate or available. The data shows that more people in total-ban states are using telehealth while fewer are traveling out of state.
Shield laws are one reason for that shift. They are state laws designed to protect clinicians who provide abortion care across state lines from states where abortion is banned or restricted. These laws do not remove every legal risk, but they have changed how abortion access works for patients who cannot travel.
Coverage And Cost Still Limit Access
Legal status is only one barrier. Cost, travel, insurance, child care, work schedules and appointment availability all affect whether a person can obtain care.
KFF reports that the national median self-pay price for medication abortion was $563 in 2023, while virtual telehealth clinics were much lower, around $150. Coverage also varies heavily by state and plan type.
| Coverage Or Cost Issue | Latest KFF Finding |
| Medication abortion median self-pay price | $563 in 2023 |
| Virtual telehealth medication abortion price | About $150 |
| Private plan restrictions | 10 states restrict abortion coverage in private plans |
| Marketplace plan restrictions | 25 states ban abortion coverage in Marketplace plans |
| State Medicaid funding beyond Hyde restrictions | 20 states use state-only funds to cover abortions under broader circumstances |
| Payment source before Dobbs | 60% of abortion patients paid out of pocket, 26% used Medicaid and 11% used private insurance |
The Hyde Amendment bars federal Medicaid funding for abortion except in cases of rape, incest or life endangerment. States can use state-only funds for broader coverage, but many do not. That leaves many patients paying directly or relying on abortion funds and travel support groups.
For broader health coverage context, NCH Stats has covered Medicaid coverage changes, which remain important because Medicaid status is tied to abortion cost, pregnancy care and postpartum access.
Health Outcomes Linked To Abortion Bans
New research published after Dobbs has moved the debate beyond legal categories. The main health finding is direct: when states ban abortion, more pregnancies are carried to term, and infant deaths rise above expected levels in some affected states.
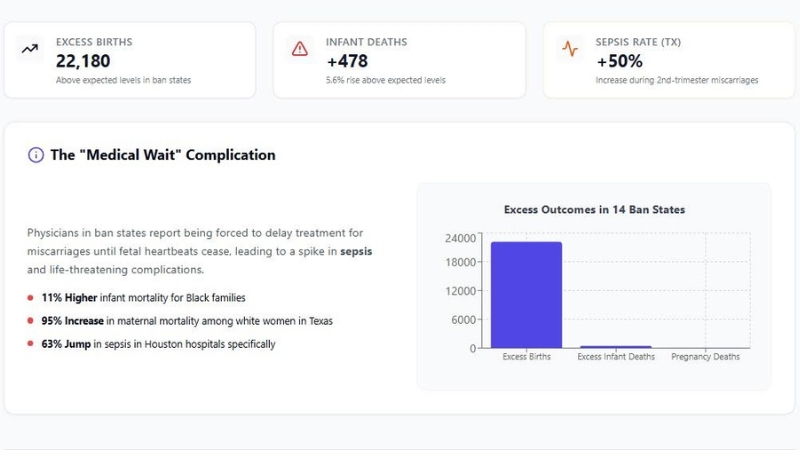
Johns Hopkins researchers reported that abortion bans in 14 states were associated with 22,180 additional live births and 478 additional infant deaths above what would have been expected without those bans.
The infant mortality study in JAMA found a 5.6% relative increase in infant mortality in states after complete or six-week bans took effect.
| Research Finding | Reported Result | Why It Is Important |
| Additional live births | 22,180 more live births than expected in 14 states | Bans changed birth outcomes at the population level |
| Additional infant deaths | 478 more infant deaths than expected | Infant mortality increased in states with bans |
| Overall infant mortality increase | 5.6% relative increase | Observed infant mortality exceeded the model’s expected rate |
| Black infant mortality | About 11% higher than expected | Existing racial disparities were amplified |
| Congenital anomaly deaths | Higher than expected | Restrictions can force continuation of pregnancies with severe fetal conditions |
| Texas impact | Texas had the largest influence on the overall infant death count | Texas imposed an early six-week ban before many other states |
These findings do not mean every state ban has the same effect. They do show that abortion policy can change births, infant mortality and emergency pregnancy care. That connection is why abortion bans are now part of public health research, not only legal reporting.
NCH Stats has also reported on maternal mortality trends, an area closely connected to emergency pregnancy care, hospital practice and state policy.
Racial And Ethnic Disparities

Abortion bans fall hardest on people who already face barriers to health care. Johns Hopkins reported higher-than-expected live births among racially minoritized people, Medicaid beneficiaries, unmarried people, younger people and residents of Southern states.
The JAMA infant mortality study found the increase was larger among non-Hispanic Black infants than other groups. The study estimated 11.81 observed infant deaths per 1,000 live births among Black infants in ban states, compared with 10.66 expected.
That is why abortion data should be read with wider demographic and health data. NCH Stats has a separate report on the Black population in the United States by county, and many total-ban states are also states with large Black populations, high poverty in rural areas and limited maternal health infrastructure.
Emergency Care Is Still One Of The Hardest Parts Of The Law
Many abortion bans say doctors can intervene to save a patient’s life or address serious physical health risks. The difficult part is timing. Doctors may have to decide how sick a patient must be before the exception clearly applies.
That uncertainty can affect miscarriage management, ectopic pregnancy treatment, severe infection, premature rupture of membranes, hemorrhage and fetal diagnoses that threaten the patient’s health. The result is not always a clean legal answer at the bedside.
For readers, the key point is simple. A state exception does not always translate into immediate hospital care. Hospital lawyers, provider licensing rules, criminal penalties, documentation requirements and fear of prosecution can shape what happens in emergency rooms.
2026 Ballot Measures Could Change The Map Again
Ballot measures have become one of the main ways abortion policy changes after Dobbs. KFF reports that voters in Missouri, Nevada and Virginia will weigh abortion measures in November 2026, while Idaho and Nebraska measures are in the signature process.
| State | 2026 Ballot Status | What The Measure Could Do |
| Missouri | On the November 2026 ballot | A legislatively referred measure would repeal the 2024 reproductive rights amendment and impose narrower abortion rules |
| Nevada | On the November 2026 ballot | Voters must approve the reproductive rights amendment a second time for it to be added to the state constitution |
| Virginia | On the November 2026 ballot, subject to litigation | Would add reproductive freedom protections to the state constitution |
| Idaho | Signature process | Proposed reproductive freedom measure could change access if it qualifies and passes |
| Nebraska | Signature process | Proposed personhood-related measure could restrict reproductive rights if it qualifies and passes |
Missouri is the state to watch most closely because voters approved abortion protections in 2024, and lawmakers placed a 2026 measure on the ballot that would reverse much of that change. Nevada is different because the state requires constitutional amendments from citizen initiatives to pass in two successive general elections.
For wider political context, NCH Stats covered red vs. blue states, and abortion policy remains one of the clearest examples of how state politics shape daily life after Dobbs.
Public Opinion Is More Supportive Than Many State Laws
Public opinion remains more supportive of legal abortion than many state laws. Pew Research Center reported in 2026 that 60% of U.S. adults say abortion should be legal in all or most cases, while 38% say it should be illegal in all or most cases.
Pew also found a gender gap: 64% of women and 55% of men said abortion should be legal in all or most cases. Support was highest among adults under 30, at 66%.
| Polling Measure | 2026 Pew Finding |
| All U.S. adults | 60% say abortion should be legal in all or most cases |
| Women | 64% say abortion should be legal in all or most cases |
| Men | 55% say abortion should be legal in all or most cases |
| Adults ages 18-29 | 66% say abortion should be legal in all or most cases |
| Adults ages 30-49 | 61% say abortion should be legal in all or most cases |
| Adults ages 50-64 | 57% say abortion should be legal in all or most cases |
| Adults age 65 and older | 57% say abortion should be legal in all or most cases |
KFF’s women’s health survey also found that 70% of women of reproductive age support a nationwide right to abortion. KFF reported broad support for emergency access, travel for abortion care and protections for doctors who provide abortions.
Why Exceptions Often Do Not Work The Way They Sound
Many abortion bans include exceptions. In practice, exceptions can be difficult to use because they require specific legal conditions, documentation, timing, provider willingness and hospital approval.
- Rape and incest exceptions can require law enforcement reporting or strict time limits.
- Health exceptions can be written narrowly or interpreted cautiously by hospitals.
- Fetal anomaly exceptions exist in some states and are absent in others.
- Emergency exceptions can leave doctors waiting until a patient condition becomes more severe.
- Criminal penalties can make physicians cautious even when a medical case appears urgent.
Legal status and medical access are not the same thing. A state can list an exception, yet patients and clinicians may still face delay, transfer, denial or legal uncertainty.
Where Care Is Still Provided And Where It Has Shifted
The national abortion total remained high after Dobbs because care moved rather than disappeared. People traveled, clinics in protective states absorbed patients, and telehealth systems expanded.
| Access Pattern | 2026 Explanation |
| Total-ban states | In-state abortion provision is limited to narrow exceptions, while many residents use travel or telehealth |
| Six-week-ban states | Some early care remains legal, but many patients discover pregnancy too late for in-state care |
| Travel states | Illinois, North Carolina, New Mexico and other states continue to serve many out-of-state patients |
| Shield-law states | Clinicians in protective states provide telehealth medication abortion to patients in restrictive states |
| Protective states | Legal access is broader, but clinic capacity, cost and appointment timing still shape care |
Guttmacher reported that Illinois provided 32,000 abortions to out-of-state residents in 2025, almost a quarter of all people nationwide who traveled for care that year. North Carolina provided almost 18,000 abortions to out-of-state patients in 2025 despite its own 12-week limit and waiting period, largely because Florida’s six-week ban changed access in the Southeast.
What Patients Usually Need To Check First
Anyone trying to understand abortion access in a specific state needs more than a map. The legal category is only the starting point.
| Question | Why It Matters |
| How far along is the pregnancy by LMP? | Many state limits are counted from the last menstrual period |
| Is there a mandatory waiting period? | A legal appointment can become too late after delays |
| Does the state require in-person counseling or ultrasound? | Two-trip rules can raise cost and travel barriers |
| Does insurance cover the care? | Many patients still pay out of pocket |
| Is telehealth legally available? | Medication abortion access depends heavily on state law and shield-law providers |
| Is the situation an emergency? | Emergency care can involve different rules and hospital review |
The answer can change quickly because state laws, court orders and ballot measures are still moving. Readers should verify current rules with a clinic, legal help organization or state policy tracker before making decisions based on a general state table.
What To Watch Next
The abortion map can still change before the end of the year. The main questions are legal, political and medical.
- Whether the Supreme Court eventually takes a final merits decision in Louisiana v. FDA on mifepristone distribution.
- Whether Missouri voters keep or repeal the reproductive rights amendment approved in 2024.
- Whether Nevada voters approve reproductive rights protection a second time.
- Whether Virginia voters add reproductive freedom language to the state constitution.
- Whether Idaho or Nebraska measures qualify for the ballot.
- Whether more state courts interpret abortion exceptions, emergency care rules or telehealth laws.
- Whether shield-law providers face more interstate lawsuits.
The legal status of abortion in 2026 is a moving target. Readers should treat state-law tables as current snapshots, not permanent rules.
Methodology
This article uses KFF state abortion policy data for the 2026 legal status categories, including total bans, six-week limits, other gestational limits and states with no gestational limit. KFF’s table reflects state policies and court decisions and lists state-by-state exceptions.
Abortion incidence and travel figures come from Guttmacher’s 2026 release and full-year 2025 Monthly Abortion Provision Study report. Those estimates include clinician-provided procedural and medication abortions, including telehealth provision to residents of total-ban states. The estimates exclude self-managed abortions not provided by U.S. clinicians and therefore undercount the full number of abortions.
Medication abortion information comes from KFF’s updated medication abortion brief. Health outcome findings come from Johns Hopkins Bloomberg School of Public Health and JAMA studies on additional births and infant mortality after abortion bans. Ballot measure information comes from KFF’s 2026 ballot initiative tracker. Public opinion figures come from Pew Research Center and KFF polling.
FAQs
How many states ban abortion in 2026?
KFF lists 13 states as abortion-ban states in 2026: Alabama, Arkansas, Idaho, Indiana, Kentucky, Louisiana, Mississippi, North Dakota, Oklahoma, South Dakota, Tennessee, Texas and West Virginia.
Is Missouri a state where abortion is illegal in 2026?
No. Missouri is not listed by KFF as a current total-ban state in the 2026 data used for this article. Missouri voters approved reproductive freedom protections in 2024, and the state is facing another abortion measure in November 2026.
What does a six-week abortion ban mean?
A six-week ban usually uses LMP, or last menstrual period. That means the clock starts before many people know they are pregnant. A six-week law can close access soon after a missed period.
Does no gestational limit mean abortion is available at every clinic?
No. No gestational limit means the state does not set a cutoff in the same way other states do. Actual access still depends on clinics, providers, cost, insurance, scheduling and medical circumstances.
Are abortion pills banned in states with abortion bans?
State abortion bans generally apply to medication abortion as well as procedural abortion. In-state providers in ban states usually cannot legally provide abortion pills except under narrow exceptions.
Why is mifepristone still in court?
Mifepristone is central to the legal fight because it is the first drug in the most common medication abortion regimen. State-led lawsuits challenge federal rules that allow telehealth prescribing and mail or pharmacy dispensing.
Why do some people travel if telehealth is available?
Telehealth is not available or appropriate for every case. Some patients are later in pregnancy, need procedural care, have medical concerns, lack a safe mailing address, or live in a situation where privacy is difficult.
Do abortion exceptions protect every emergency case?
No. Exceptions vary by state and can be difficult to apply. Hospitals and doctors may require legal review, documentation or worsening medical conditions before acting under an exception.
Why do abortion bans affect infant mortality?
Research after Dobbs found that bans were associated with more live births and higher-than-expected infant deaths in affected states. One reason is that some pregnancies with severe fetal conditions continue because abortion access is restricted.
Bottom Line
As of 2026, abortion is banned in 13 states: Alabama, Arkansas, Idaho, Indiana, Kentucky, Louisiana, Mississippi, North Dakota, Oklahoma, South Dakota, Tennessee, Texas and West Virginia. Four more states, Florida, Georgia, Iowa and South Carolina, ban abortion at about six weeks LMP.
The national picture is more complicated than the ban list alone. Guttmacher estimates 1,126,000 clinician-provided abortions in 2025, almost unchanged from 2024. Travel for care declined, while telehealth provision to people in total-ban states increased. Medication abortion, mifepristone litigation, shield laws and 2026 ballot measures now shape access as much as clinic maps do.
The main takeaway for readers is clear: abortion access in the United States depends on state law, pregnancy timing, money, travel, telehealth availability and the next round of court and ballot decisions.