

One in four U.S. children wore glasses or contact lenses in 2019, according to CDC data tied to the National Health Interview Survey.
Among children ages 2 to 17, 25.3% used corrective lenses, showing that vision correction is a common part of childhood health.
Clear vision is not only a routine back-to-school concern. A child who cannot see well may struggle with reading, classwork, sports, social development, and daily confidence.
Vision care also connects to health equity, because screening, eye exams, and access to corrective lenses are not evenly available to every child.
CDC data show that corrective lenses are common among American children, especially older children and girls.
Evidence tied to pediatric myopia, geographic gaps, and vision-loss risk also points to a growing public-health challenge for families, schools, clinicians, and communities.
CDC Data – How Many Children Wear Glasses or Contacts?

CDC findings used 2019 National Health Interview Survey data.
Estimates relied on parent or household answers to a question asking if a child wears eyeglasses or contact lenses.
Usage was low among preschool-age children, then rose sharply during school-age years and adolescence.
Age groups showed a steep rise as children moved into school and teenage years:
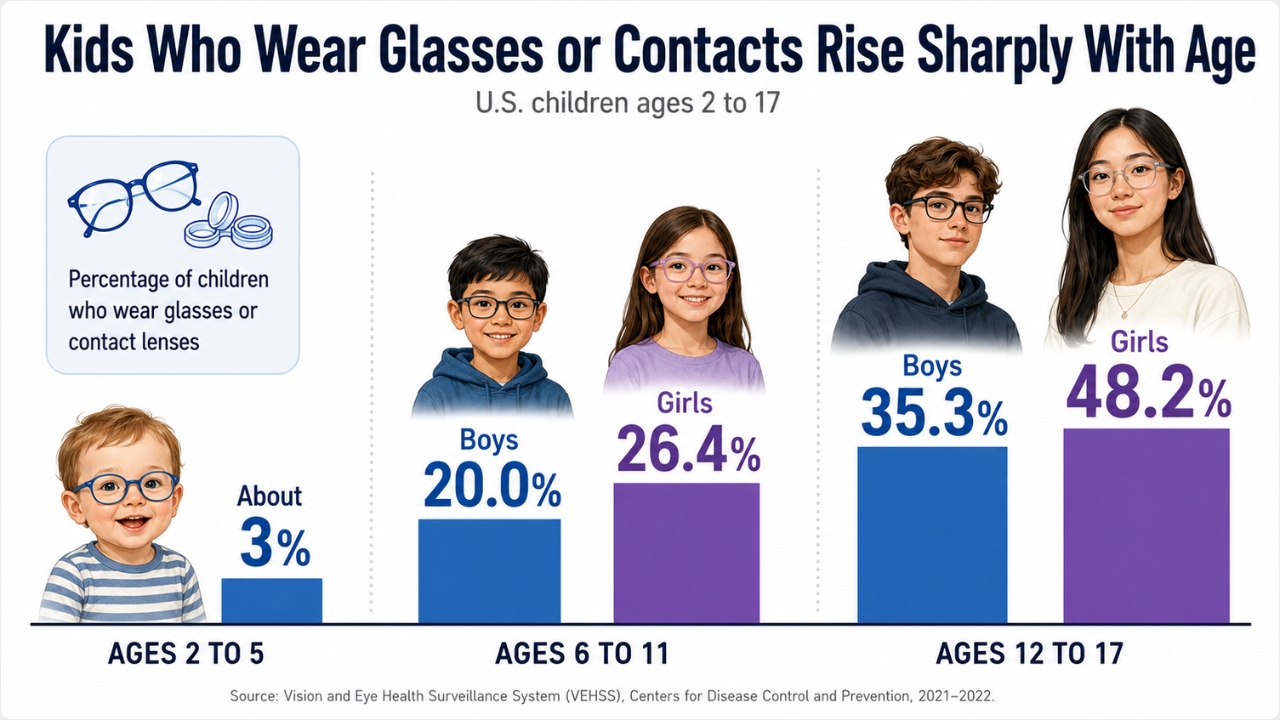
Age shows one of the strongest patterns in the data. Corrective lens use becomes much more common as children get older.
By adolescence, glasses or contacts are especially common, with nearly half of girls ages 12 to 17 using them in 2019.
Why Nearsightedness Is a Growing Concern
Glasses and contacts can correct several vision issues, but myopia is one major reason children need them.
In adulthood, some people with stable nearsightedness may consider vision correction procedures such as SMILE eye surgery, which is designed to treat myopia with or without astigmatism.
Myopia, also called nearsightedness, makes distant objects look blurry while close objects may look clear.
Reported estimates indicate that 40% of U.S. children ages 6 to 19 are nearsighted.
That number places myopia among the most important pediatric vision concerns in the country.
Myopia is not only an inconvenience managed with lenses. Severe or progressive myopia can increase the risk later in life for several eye problems:
Early childhood onset can be especially concerning because more years of eye growth may allow progression to continue. Global projections add urgency. Researchers have projected that about half of the world’s population could be myopic by 2050 if current trends continue. For children, families, and health systems, myopia is increasingly viewed as a long-term eye-health issue, not just a reason to update a glasses prescription. Girls were more likely than boys overall to wear glasses or contacts in the CDC data. Among very young children, ages 2 to 5, no major sex difference appeared. Gaps became more visible in ages 6 to 11 and widened further among ages 12 to 17. Behavior, biology, and access to care may all play roles. CDC data reports the pattern, but they do not fully explain the cause. More research is needed to separate differences in eye development, diagnosis, family follow-up, and health-care access. Behavioral patterns are often discussed as part of rising pediatric myopia. Close-range visual tasks, including reading, homework, phone use, tablet use, and computer use, may contribute to risk when they take up long stretches of time. Reduced outdoor time is another major concern. More time outside appears linked with lower myopia risk or slower progression for some children. Bright outdoor light may help regulate eye growth, which may reduce the chance that an eye grows too long and causes nearsightedness. Pandemic-era changes brought new attention to the issue. Home confinement and remote learning increased children’s screen exposure and reduced normal outdoor routines. During that period, researchers reported increased myopia onset and faster progression, especially among younger school-age children. Children still need reading, learning, and digital tools, but long close-up sessions should be broken up. Daily outdoor time may support eye health, along with regular vision screening and timely eye exams when a child shows signs of trouble seeing. Corrective lenses address many childhood vision problems, but not every condition can be fixed with glasses or contacts. CDC fast facts estimate that about 6.8% of U.S. children younger than 18 have a diagnosed eye and vision condition. Nearly 3% of children younger than 18 have blindness or vision impairment, defined as trouble seeing even while wearing glasses or contacts. That distinction matters because many children have correctable refractive errors, while others have visual acuity loss or more serious eye conditions that need additional care. Untreated vision problems can affect school performance, development, safety, and quality of life. A child who struggles to see the board, read small print, follow visual instructions, or take part in activities may fall behind without anyone quickly recognizing the reason. Early detection matters. Vision screening can identify children who need a full eye exam, and eye exams can guide treatment, lenses, monitoring, or specialty care. For many children, timely care can improve daily functioning and reduce the chance of avoidable harm. Children’s vision health varies across communities. County and state-level mapping tools show visual acuity loss, blindness, and access to eye care among U.S. children, while also comparing outcomes with income, disability status, provider availability, educational measures, and screening rules. More than 600,000 U.S. children live with uncorrectable visual acuity loss or blindness. Millions more have vision problems linked to uncorrected acuity issues that could be resolved with glasses or contacts. Poverty is closely correlated with childhood vision loss. Families with limited income may face barriers tied to transportation, insurance coverage, appointment availability, out-of-pocket costs, and follow-up care after screening. Racial and ethnic disparities also appear in national vision data. Non-Hispanic Black children are reported to have the highest rates of vision loss and blindness. Such gaps show that pediatric vision health is tied not only to biology, but also to access, community resources, and broader social conditions. One in four children has #vision problems that affect their learning. #kidsinglasses #edu #Sight #Learn #See #eyetips #glasses — EYEFUNC Eyewear (@EYEFUNC) November 1, 2012 One in four U.S. children ages 2 to 17 wore glasses or contacts in 2019, and rates rose steeply by age. Among teenagers, corrective lenses were especially common, with 35.3% of boys and 48.2% of girls ages 12 to 17 wearing them. Corrective lenses are common, but children’s vision health is not evenly distributed. Myopia trends, screen habits, near work, outdoor time, poverty, provider access, screening practices, and follow-up care all shape a child’s ability to see well. For families, schools, pediatricians, eye-care providers, and public-health agencies, the numbers point to a clear need for early screening, accessible care, and attention to the children most likely to be missed.
Gender Differences in Children’s Vision Correction

Screen Time, Near Work, and Outdoor Time
Vision Problems Not Fixed by Glasses Alone
Geographic and Socioeconomic Disparities

FAQs
Closing Thoughts





