Medicaid is a major source of coverage for people with mental health conditions and substance use disorders.
For many adults, it pays for therapy, psychiatric medication, addiction treatment, recovery support, and crisis care.
New Medicaid work and reporting requirements would add another layer of eligibility checks.
Supporters frame these rules as a way to encourage work and reduce spending, but for people with behavioral health needs, added paperwork can become a barrier to care.
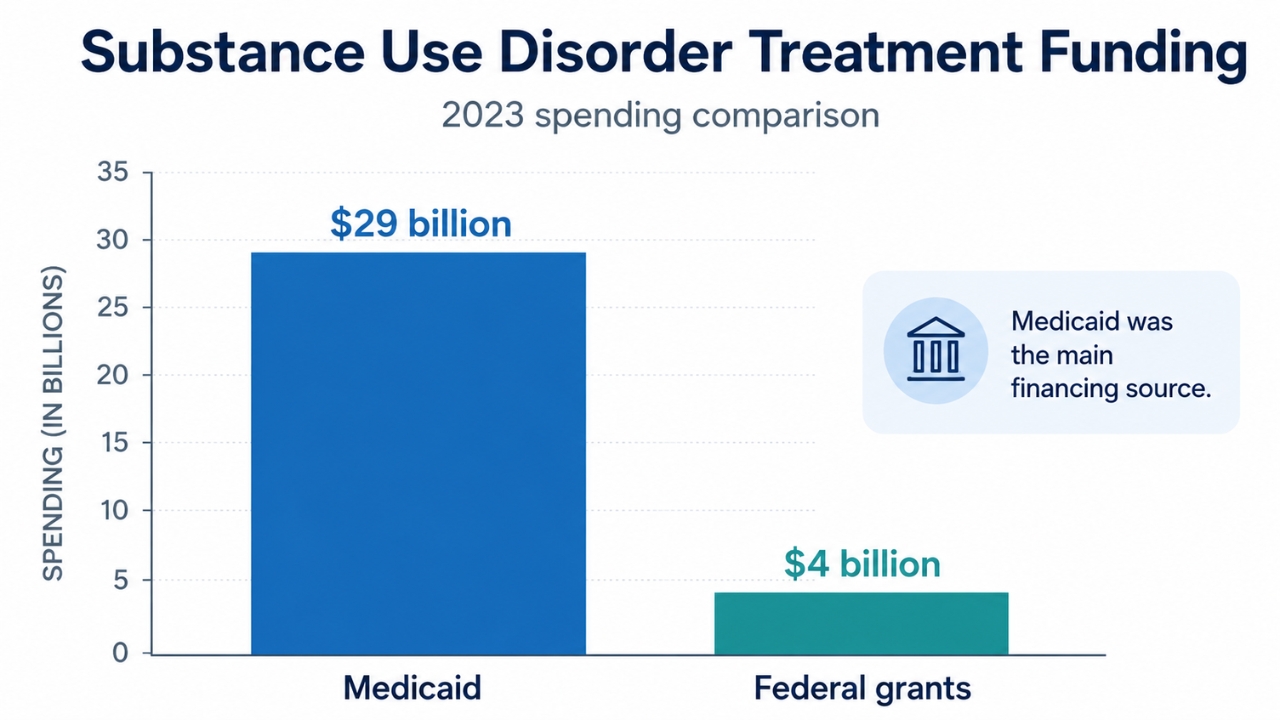
Coverage loss on that scale would affect people who already face serious gaps in mental health and addiction treatment. Medicaid is one of the largest payers for behavioral health care in the United States. It pays for one-quarter of all U.S. spending on mental health and substance use disorder treatment services. Its role is especially important because many people with behavioral health needs rely on Medicaid, not private insurance, to access care. Many adults with behavioral health conditions qualify through the ACA expansion rather than disability-based eligibility. Among Medicaid-covered adults with diagnosed behavioral health conditions, ACA expansion is the main pathway for 59% of those with substance use disorders, 61% of those with opioid use disorders, 51% of those with any mental health disorder, and 45% of those with serious mental illness. Losing coverage can interrupt medication, counseling, addiction treatment, and recovery services. Access to care matters because treatment often includes several connected services, not just one appointment. Programs like Elevate Recovery MA provide addiction and mental health treatment options that can include outpatient care, counseling, dual-diagnosis support, medication-assisted treatment, relapse prevention, and aftercare planning. When Medicaid coverage is interrupted, people may lose access to the kind of ongoing support that helps stabilize recovery. Even short gaps can worsen symptoms, delay care, and increase the chance of crisis treatment. Implementation would begin no later than December 31, 2026. People who fail to prove compliance or exemption could be denied coverage or removed. Some exemptions are included for people with substance use disorders or disabling mental disorders. Participation in a substance use disorder treatment program is also listed as an exemption. Risk comes from unclear definitions. The current language does not clearly define which mental health diagnoses count as disabling. Future federal guidance and state implementation would shape how exemptions apply. Schizophrenia, psychotic disorders, and bipolar disorder might qualify, but that has not been clarified. People with serious depression, anxiety, trauma-related disorders, or addiction could still struggle to prove that their condition fits the exemption standard. Exemptions may not work if people cannot claim them easily. Some enrollees may need to self-report, submit documentation, provide treatment records, or get a provider to certify their condition. Policy language does not specify if states must use available data to verify exemptions automatically. It also does not clearly say if individuals must report their condition or provide documents themselves. Claims data may help identify some eligible people, but it can lag. Claims may take weeks or months to process, which could delay the identification of people who should be exempt. Behavioral health symptoms can make reporting harder. Difficulty concentrating, low energy, anxiety, trouble planning, feeling overwhelmed, and difficulty managing stress can interfere with forms, online portals, notices, and deadlines. Coverage loss under these rules may not show unwillingness to work. It may show that someone could not complete an administrative process. People with substance use disorders face a high risk under work and reporting requirements because addiction can affect work stability, housing, transportation, health, and access to documentation. Some proposals exempt people in addiction treatment programs. That exemption may miss many people who need help. Federal SNAP treatment-program exemptions are limited to people in private nonprofit treatment facilities and community mental health centers. Those facilities account for less than half of substance use disorder treatment facilities in the United States. Many people with substance use disorders are not in treatment. That creates a documentation problem. A person may have a serious addiction but no diagnosis, provider note, or treatment record. If proof is required, that person may need Medicaid-covered care to get the documentation needed to keep Medicaid. A person who fails a work requirement because of substance use may lose coverage before seeing a provider for diagnosis or treatment referral. That can delay treatment and raise the risk of relapse, overdose, emergency care, or justice-system involvement. Co-occurring conditions increase the risk. Many people with substance use disorders also have mental health or physical health conditions. If only addiction treatment program participation counts as an exemption, people may still lose access to care for depression, anxiety, chronic pain, infectious disease, pregnancy-related needs, or other conditions. Medicaid also carries far more of the addiction-treatment financing burden than federal grants: Grant programs can support targeted services, but they cannot replace Medicaid as the main financing source for addiction treatment. Work and reporting requirements would add repeated administrative tasks for Medicaid enrollees. Patients may need to track hours, submit forms, collect pay records, request exemptions, and provide medical documentation. For people managing depression, anxiety, psychosis, addiction, trauma, or unstable housing, small administrative failures can lead to major consequences. A missed notice, lost password, delayed appointment, or broken phone can become a coverage problem. Providers may also face added paperwork. Clinicians may be asked to decide if a patient is unfit to work or if a condition qualifies for an exemption. In mental health and addiction care, that decision can affect access to treatment with life-or-death stakes. New Hampshire’s work requirement waiver offers one example. Adults who self-attested to being medically frail still had to obtain certification by a medical professional. Reports described that process as difficult for enrollees and complicated for providers. States would also need to spend money building or expanding compliance systems. That could include data matching, notices, online portals, staffing, appeals, documentation review, and renewal procedures. Money used for those systems would not directly expand therapy, addiction treatment, crisis response, or provider capacity. Medicaid work requirements are part of a wider set of policy changes affecting behavioral health care. Concerns include Medicaid funding cuts, proposed reductions to federal mental health agencies, and weaker enforcement of mental health parity rules. The “One Big Beautiful Bill” includes almost $1 trillion in cuts to Medicaid over the next 10 years. https://t.co/Tyg7dRhabv — More Perfect Union (@MorePerfectUS) July 6, 2026 H.R. 1, passed on July 4, 2025, cut federal Medicaid funding by 15%, or $1 trillion over 10 years. Behavioral health care would be hit hard because Medicaid beneficiaries are more likely to have behavioral health disorders than people with private insurance or no insurance. Medicaid also pays for one-quarter of behavioral health spending. Federal mental health funding has also faced instability. SAMHSA terminated hundreds of mental health and substance use disorder grants totaling about $2 billion on January 13, 2026. Funding was reinstated the next evening after bipartisan pushback. The proposed restructuring of federal mental health agencies raised more concern. Plans included dissolving SAMHSA and HRSA into a new Administration for a Healthy America, along with a proposed $1 billion cut to these programs. Combined effects could mean fewer appointments, fewer providers, higher out-of-pocket costs, longer delays, and more people waiting until a crisis before getting care. Supporters may argue that work requirements encourage employment and preserve Medicaid for people most in need. Behavioral health data complicates that claim. Many adults with mild or moderate mental health or substance use conditions already work or participate in qualifying activities. Many also rely on Medicaid-covered treatment and medications to keep working. Coverage loss caused by paperwork problems does not create employment. It can make employment harder. Poor health is linked to a greater risk of job loss, while affordable health care can help people get and keep work. Work reporting requirements in public benefit programs have not led to clear employment gains. Instead, they have often led to coverage loss. People can lose benefits because they cannot complete the reporting process, not because they are ineligible or refusing to work. For someone with depression, losing medication can make daily functioning harder. For someone with opioid use disorder, losing treatment can raise the risk of relapse or death. For someone with anxiety or bipolar disorder, losing stable care can disrupt work, housing, and family life. A policy meant to support work can undermine work when it removes health coverage that helps people stay stable. Reduced Medicaid access can interrupt therapy, psychiatric medication, medication for opioid use disorder, counseling, case management, and crisis support. Those interruptions can worsen symptoms and increase risk. Care gaps are already severe. Two-thirds to three-quarters of people identified as meeting criteria for a mental health disorder reported not receiving treatment. Adding reporting barriers would land on top of that existing shortage. Provider access is also strained. Behavioral health insurance reimbursements are, on average, 22% lower than reimbursements for medical or surgical office visits. Lower payments can discourage providers from joining insurance networks. Untreated behavioral health conditions carry major social and economic costs. One study found that untreated mental illness costs Indiana $4.2 billion, about 1% of the state’s gross domestic product, in direct, indirect, and societal costs. Addiction treatment interruptions can be deadly. Stopping medication for opioid use disorder significantly increases mortality risk, with a six-fold greater risk of death in the four weeks after treatment discontinuation. Overdose deaths have recently decreased, but the United States is still losing close to 100,000 lives every year. New barriers to care could put more people at risk during an ongoing addiction crisis. New Medicaid work and reporting requirements could make mental health and addiction treatment harder to access, even for people who are supposed to be exempt. Medicaid is central to behavioral health care. It covers nearly one-third of adults with mental health disorders and one-fifth of adults with substance use disorders. Coverage loss would directly affect people who already face major treatment gaps. Policymakers should protect continuous Medicaid coverage and strengthen mental health and substance use disorder treatment. People dealing with mental illness or addiction need stable access to care, not more ways to lose it.
Medicaid’s Role in Mental Health and Addiction Care

What the New Medicaid Requirements Would Do
Under the House-passed bill discussed by policy analysts, many ACA Medicaid expansion adults would need to complete 80 hours per month of work or qualifying activities unless they qualify for an exemption.
Why Exemptions May Not Protect People Who Need Care

Special Risks for People With Substance Use Disorders
Administrative Burdens on Patients, Providers, and States
Broader Policy Changes Could Further Reduce Access
Counterargument and Response

Consequences of Reduced Access
Summary